
What Is Lipedema? Why Millions of Women Are Being Told "Just Lose Weight" — When That's Not the Problem
You've tried every diet. You've done the workouts. Your upper body responds. Your lower body doesn't budge.
Doctors have called it "baby weight." They've called it obesity. They've handed you calorie charts and sent you on your way.
But here's what nobody told you: it might not be fat. It might be lipedema — and it's not your fault.
So, What Exactly Is Lipedema?
Lipedema (pronounced lip-ih-DEE-mah) is a chronic condition involving the abnormal accumulation of fatty tissue — primarily in the hips, thighs, buttocks, and sometimes the arms. It is almost entirely a women's condition, and it is far more common than most people realize.
Estimates suggest lipedema affects somewhere between 6% and 11% of women worldwide — possibly higher in the U.S. and Europe. That's potentially millions of women walking around without a diagnosis, without answers, and without proper care.
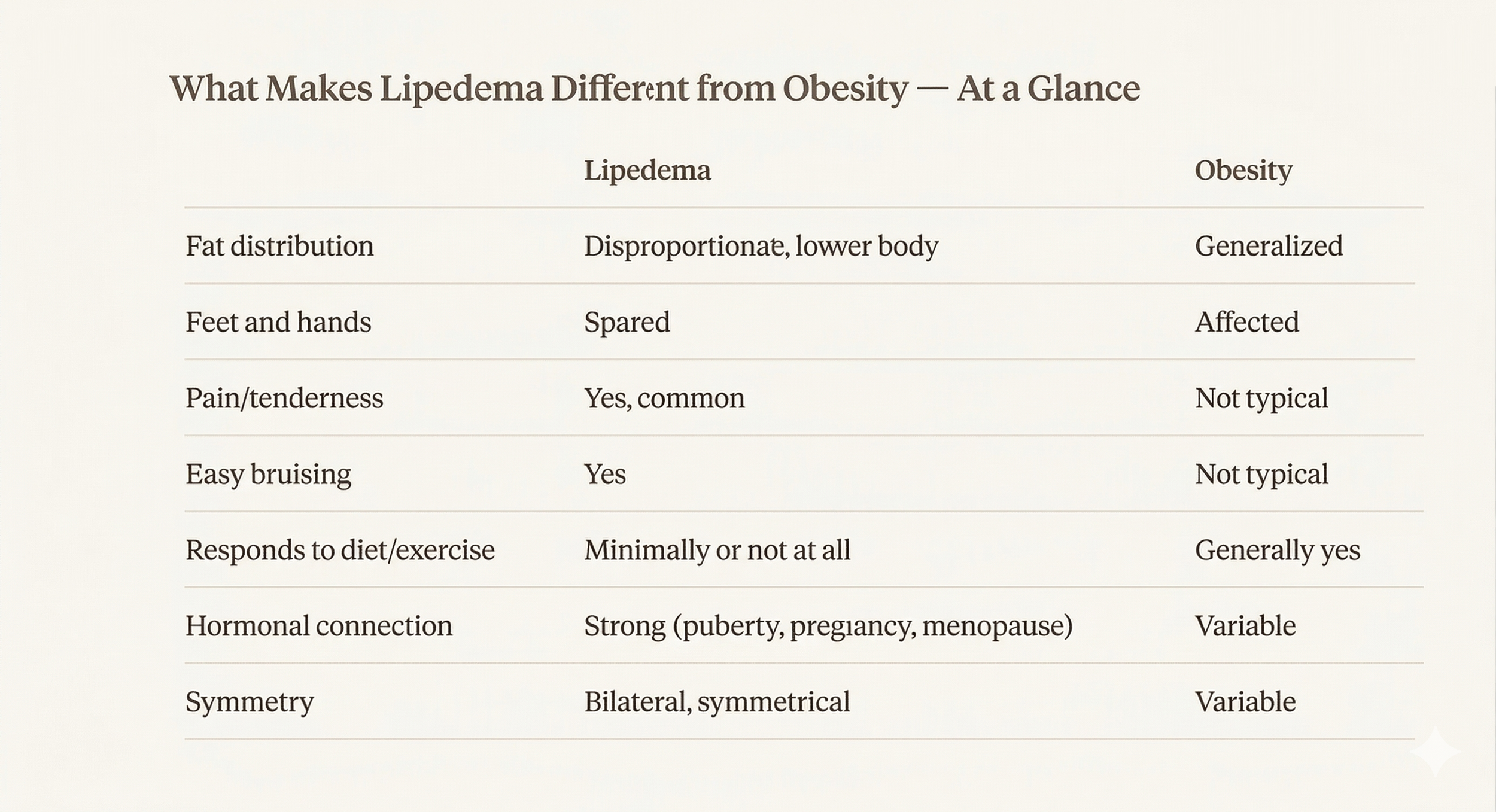
Here's what makes lipedema unique and what makes it so frequently missed:
The fat accumulation is symmetrical and disproportionate — your lower body enlarges while your upper body may stay relatively slim
The affected tissue is painful and tender to the touch — pressing on lipedema tissue hurts in a way that regular fat does not
You bruise easily, often without a clear reason
The swelling worsens throughout the day and is influenced by hormonal changes (puberty, pregnancy, menopause)
The feet and hands are typically spared — a key clinical clue
Diet and exercise do not reduce it — and this is perhaps the most important distinction of all
That last point is critical. Lipedema fat is physiologically resistant to weight loss. You can eat well, exercise consistently, and watch your upper body transform while your lower body stays exactly the same — or gets worse. This is not a willpower problem. This is biology.
Why Is Lipedema So Commonly Mistaken for Obesity?
This is where things get painful — not just physically, but emotionally.
Research shows that up to 50% of women with lipedema are initially misdiagnosed as obese. Half. That means for every two women sitting in a doctor's office describing painful, disproportionate swelling that doesn't respond to diet, one of them is being sent home with the wrong answer.
Why does this keep happening?
1. Lipedema isn't taught in most medical schools. The condition is largely absent from standard medical curricula and specialty training programs. Many physicians have simply never been trained to recognize it.
2. There is no definitive test. Lipedema is a clinical diagnosis based on physical examination and patient history. Without a clear lab value or imaging standard, it's easy for providers to default to a more familiar explanation — obesity.
3. BMI is a poor tool here. Most of us are conditioned to trust the BMI scale. But in lipedema, BMI is misleading. A woman may have an elevated BMI purely because of the disproportionate tissue accumulation in her lower body — not because of generalized weight gain. Interestingly, research has also found that women with lipedema tend to have lower rates of diabetes and normal blood pressure, despite elevated BMI — which doesn't fit the typical obesity profile at all.
4. The conditions can coexist. This is where it gets complex. Obesity and lipedema can occur together, which makes it harder for clinicians to distinguish where one ends and the other begins. But treating lipedema as if it were solely an obesity issue means patients spend years in programs that were never designed to help them.
The result? Diagnosis can be delayed by up to 10 years. A decade of being told the wrong thing. A decade of failed diets, shame, and worsening symptoms.
"I Just Thought I Was Built This Way"
That phrase comes up again and again from women who eventually receive a lipedema diagnosis.
They spent years — sometimes decades — believing their body was the problem. That they weren't trying hard enough. That if they just found the right program, the right diet, the right doctor, things would change.
What they didn't know was that their lymphatic system and connective tissue were working against them in a way that no caloric deficit was going to fix.
Lipedema is not a lifestyle disease. It's thought to have a strong hormonal and genetic component, often first appearing or worsening during puberty, pregnancy, or menopause — moments when estrogen fluctuates significantly. Women often describe noticing the change seemingly overnight: suddenly their body shifted in ways they couldn't explain and couldn't reverse.
That's not a failure of effort. That's a physiological response.
What Are the Stages of Lipedema?
Lipedema is progressive, which means it can worsen over time without proper support. It is typically classified into four stages:
Stage 1: Skin surface is smooth but subcutaneous fat tissue is enlarged. Skin may feel soft and slightly spongy.
Stage 2: The skin surface becomes uneven, with a mattress-like texture. Fatty nodules can be felt underneath.
Stage 3: Large overhangs of tissue form, particularly around the thighs and knees. Mobility may begin to be affected.
Stage 4: Lipedema has progressed to involve the lymphatic system as well, a combined condition called lipo-lymphedema. Swelling becomes more severe and complex to manage.
The earlier lipedema is recognized and supported, the better the outcomes. This is why awareness matters so much.
How Does the Lymphatic System Factor In?
Here's where my work at MBODE connects directly to what's happening in lipedema.
The lymphatic system is your body's fluid regulation network. It's responsible for clearing excess fluid, inflammatory byproducts, and waste from your tissues. In lipedema, the lymphatic vessels in the affected areas are under constant mechanical pressure from the enlarged fatty tissue — and in later stages, they begin to dysfunction.
When lymphatic drainage is compromised, fluid builds up. Inflammation increases. Tissue becomes harder, more fibrotic, and more painful. The swelling worsens throughout the day because gravity adds to the fluid load that a struggling lymphatic system can't clear effectively.
This is why manual lymphatic drainage (MLD) is one of the primary conservative treatment approaches recommended for lipedema. It's not a luxury service. For someone with lipedema, it is a medical necessity.
The MLIM™ Method we use at MBODE goes further — integrating lymphatic work with fascial and nervous system support to address not just fluid movement, but tissue quality, inflammation regulation, and the body's overall capacity to heal.
What Can Actually Help?
If you suspect you have lipedema, here's what the current evidence supports:
Conservative management:
Manual lymphatic drainage (MLD) to reduce fluid buildup and inflammation
Compression therapy (fitted compression garments worn daily)
Low-impact movement that supports lymphatic flow — walking, cycling, swimming
Anti-inflammatory dietary approaches, including ketogenic and low-carbohydrate diets, which have shown symptom improvement in several studies
Complete decongestive therapy (CDT) from a trained lymphatic therapist
Surgical options (in advanced cases):
Tumescent liposuction specifically designed for lipedema — this is different from cosmetic liposuction and requires a surgeon experienced with the condition
Post-surgical lymphatic support is critical to protect the lymphatic system during recovery
What doesn't work (and may make things worse):
Standard calorie-restriction diets targeting lower body fat
Aggressive, high-impact workouts that increase inflammation
Ignoring the symptoms and hoping they resolve
Getting a Diagnosis: What to Ask For
If you recognize yourself in this post, here are your next steps:
Find a provider familiar with lipedema. This may mean seeking out a specialist in vascular medicine, lymphology, or a dermatologist with lipedema training. Your primary care doctor may not be the right first stop.
Request a clinical evaluation focused on lipedema criteria — not just a BMI assessment. Key signs include bilateral symmetry, sparing of the feet, tenderness, bruising, and your history with diet and exercise.
Keep a symptom journal. Note when swelling is worse, pain levels throughout the day, how your body responds to food and movement, and your hormonal timeline (when did changes first appear?).
Find a community. Lipedema advocacy organizations have grown significantly in recent years. Other women who've navigated this journey are often the best guide to finding knowledgeable providers.
Seek lymphatic support. Whether or not you have a formal diagnosis yet, working with a skilled lymphatic therapist can help manage your symptoms, reduce inflammation, and give your body the support it needs while you seek answers.
You Deserve Answers — Not Assumptions
The women I work with at MBODE often come to me after years of being dismissed. They've internalized the idea that their body is the problem, that their persistence isn't enough, that something is fundamentally wrong with them.
That narrative is wrong. And it's harmful.
Lipedema is a real, recognized, physiological condition. The World Health Organization has classified it as a distinct disease in its international coding system. Research on it is growing. Awareness is building. You are not imagining it.
If your body has been telling you something doesn't add up — if the weight loss narrative has never fit your experience — trust that instinct. Seek answers. Find providers who are willing to look deeper.
And know that the right kind of support — clinical, compassionate, and grounded in how your body actually works — can make a profound difference.
Mahalath Moore is a licensed massage therapist with over 12 years of experience in post-surgical recovery, advanced lymphatic therapy, and lipedema care. She is the founder of MBODE Recovery in the Atlanta metro area and creator of the MLIM™ (Manual Lymphatic Integration Method™).
If you have questions about lipedema support or lymphatic therapy, schedule a consultation with MBODE Recovery.
Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.